
Assistive Technology
Occupational Therapy is known for its comprehensive evaluation to help individuals re-engage in their daily occupations. Many individuals experience different functional disabilities that occur due to aging, experiencing traumas, or being diagnosed with a neurological disorder. OT considers the need of individuals to use Assistive technology (AT) in order to improve their functional independence level. AT is characterized by items, equipment, or devices used to assist with difficulties in functioning to complete activities of daily living. It is considered as a last choice to help the patient improve independency after reaching the plateau. These devices can range from the electronic devices to something as simple as a piece of paper with a pencil to aid in communication. This technology can be given for Patients with different difficulties such as, musculoskeletal abnormalities, sensory deficits, and cognitive issues.
-
OT provides services that assist people with disabilities to use assistive technology devices. These services work together to fit the technology solutions with the individuals’ situations.
-
The group of services work for:
-
Evaluating
-
Selecting, designing, customizing
-
Providing devices
-
Maintaining, repairing
-
Coordinating
-
Training
-
Technical assistance
-
Assistive technologies are characterized in continuum to match the patients’ abilities and tasks.
-
Levels of the continuum:
-
No-tech
-
Low-tech
-
Medium-tech
-
High-tech
-
Represented by the procedures, services and existing tools in the environment that do not involve the use of devices or equipment.
Examples:
-
Highlighter pens & tapes
-
Specialized paper (Raised line / Contrasting line)
-
Reading and writing guides
-
Picture cards
-
Enlarged worksheets
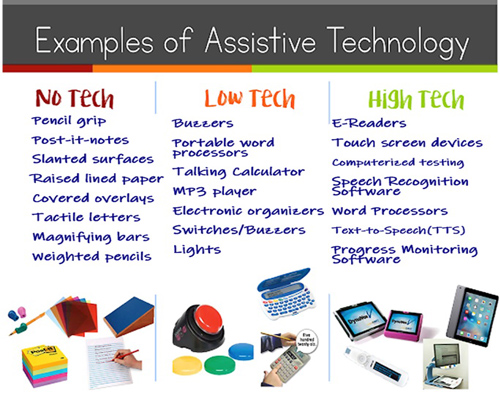
Simple items that are easy to get and repair.
Examples:
-
Adapted spoon handles
-
Non-tipping drinking cups
-
Velcro fasteners.
-
Talking calculators
-
Stand-alone switches
_edited.png)
More complicated devices, but used independently.
Examples:
-
Adaptive computer peripherals (alternative keyboards)
-
Tape recorder
-
Word processor
-
Dictionaries and Spell checker
-
Switches to use with communication devices or computers
-
Wheel chairs
Very sophisticated communication and environmental control devices.
Examples:
-
Environmental control devices
-
Software such as text readers, screen readers, voice recognition systems
-
Augmentative communication device
-
Robotics
-
Voice recognition
-
Power wheelchairs
-
Smart technology

1. The individual is referred to the AT area
2. An OT assesses the individual (according to ICF approach)
-
Detailed demographic data (Name, age, nationality, Diagnose)
-
Reasons for referral
-
History (Past, present, medical)
-
Precautions regarding the individual’s status
-
Prognosis of the disorder
-
Assessing current individual’s abilities:
-
Upper and lower extremities muscle weakness
-
Limited upper and lower extremities ROM
-
Limited head movements
-
Incoordination
-
One handedness
-
Memory dysfunction
-
Sensory dysfunctions
-
3. Giving suggestions for suitable assistive technology
-
Effectiveness (Does the device help the patient and improve their independence?)
-
Learnability (Is the patient able to understand how to use the device?)
-
Safety (Is the device safe?)
-
Affordability (Can the patient afford the cost?)
4. Trial session to evaluate the suitability of the AT
5. The patient receives the AT
6. Adapting individual to the AT and make modifications to perfectly suit them
7. Training the individual on the usage of the AT
8. Reevaluation to assure effectiveness of the device after a period of time
-
Daily living equipment (DLE)
-
Home management
-
Communication Technology (AAC)
-
Computer access
-
Driving and transportation
-
Safety Technology
-
Prosthetics (Splints)
-
Mobility technologies
-
Sensory aids


































































































Splint is a device that is temporary applied to immobilization, control, or support any part of the body. The terms splints, orthoses, and braces are used interchangeably.
Goals of Splints:
-
The splint serves as the external force to counteract the imbalances of the internal forces.
-
Support
-
Stabilize
-
Mobilize
-
Aid in healing
-
Prevent contractures
-
Improve independence in activities of daily living
-
Categories of Splints:
1. Static splints
2. Dynamic splints
3. Static progressive splints (Serial static splints)
Static Splints
A splint that is molded to maintain the tissue in one position and has no movable parts.
May be used to:
-
Relive pain
-
Position and maintain joint alignment
-
Prevent adaptive shortening of soft tissue
-
Correct soft tissue contractures
-
Immobilize a joint or limb following trauma
Examples:
-
Static CMC Splint
-
Static extension Splint
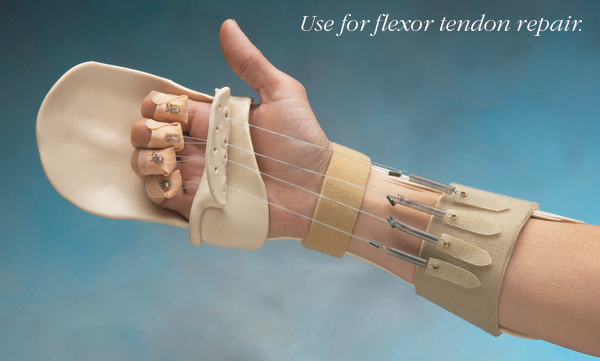
Dynamic Splints
A splint that applies force and movement to a joint(s).
Dynamic splints have three parts:
-
Splint base
-
Dynamic traction force
-
Outrigger.
May be used to:
-
Assist weakened muscles
-
Substitute for lost muscle function
-
Minimize adhesions formation
Static Progressive Splints (serial static splints)
Splints that are similar to dynamic splints, but without movable components. They Apply low-load to the joint while maintaining the tissue at its maximum length. It should be worn for extended periods of time so that the tissue adapt “grow” to its new length
May be used to:
-
Increase range of motion.
-
Correct soft tissue contractures.
-
Maintain improvement obtained through other forms of treatment, such as passive stretching.
Common Splints:
















Properties of Splints:
-
Rigidity
-
The strength of the material
-
High rigidity does not bend easily. Used for:
-
Large joints
-
Spasticity
-
-
-
Memory
-
The material ability to return to its original shape and size when re-heated
-
Material with excellent memory usually takes longer to harden
-
-
Drape-ability (Conformability)
-
Material ability to shape around and mold over contours of an extremity
-
Disadvantages:
-
Prone to fingerprints of therapist
-
Poor memory
-
Stretches and "grows"
-
Requires light touch
-
Requires cooperative patient
-
-
Degree of conformability
-
Maximum conformability (Minimum resistance to stretch)
-
Moderate conformability
-
Maximum control (Maximum resistance to stretch)
-
-
-
Bonding & Coating
-
The material ability to stick to itself or to other material when heated
-
Coated material do not bond without removing the coating
-
Advantage:
-
Can attach extra piece to splint
-
-
Disadvantage:
-
Difficult to take apart if the material folds
-
-
-
Working Time
-
The amount of time the material takes to cool
-
Beginners in splint making should start with long work time materials
-
Consider material working time based on the case to be splinted:
-
Incompliant child
-
Hard to maintain position
-
Spasticity
-
-
-
Thickness
-
Thinner materials are better for small joints
-
Thinner material have very short working time
-
-
Perforation
-
Allows better ventilation of the skin
-
Ideal for warm or humid climate
-
Splint Accessories:
-
Sticky-backed Velcro
-
Bonds best when heated (dry heat)
-
Should Round the corners to prevent catching with external materials
-
-
Padding
-
Bonds best when heated (dry heat)
-
Makes the splint smaller and tighter
-
Absorbs moisture and odor
-
Requires frequent replacement
-
Anatomical Landmarks:
-
Arches of the Hand
-
Maintain arches within the splint as they are functionally significant
-
Arches are:
-
Longitudinal Arch
-
Proximal Transverse Arch
-
Distal Transverse arch
-
-
-
Try not to splint unaffected joints.
-
Creases of the Hand
-
Clear the creases of mobile joints to allow full movement of the joint
-
General Pressure Precautions:
-
A conforming fit reduce unequal pressure
-
Avoid pressure over bony prominences
-
Use padding over bony prominence before splinting.
-
Padding afterward will increase pressure
-
Smoothed, rolled or rounded edges reduce pressure sores
-
Round corners to avoid sharp points.
Wearing Instructions:
-
The patient should wear the splint for about an hour, then remove the splint and check for red areas.
-
Redness should not last for more than 20 minutes after splint removal.
-
-
Keep in mind areas of impaired sensation
-
Splint cannot be worn for 24 hours, it should be removed for hygiene and exercises.











Click
















































































case 1
case 2
-
Cook, A. M., & Hussey, S. M. (1995). Assistive technologies: Principles and practice. St. Louis: Mosby
-
For purchase: click here
-